Tendon inflammation disease of the elbow
Medical condition
| Golfer's elbow
|
|---|
| Other names
| Medial epicondylitis
|
|---|
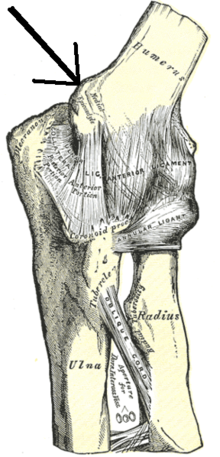 |
| Left elbow-joint, showing anterior and ulnar collateral ligaments. (Medial epicondyle labeled at center top.)
|
| Specialty
| Orthopedics
|
|---|
Golfer's elbow
, or
medial epicondylitis
, is
tendinosis
(or more precisely
enthesopathy
) of the medial
common flexor tendon
on the inside of the
elbow
.
[1]
It is similar to
tennis elbow
, which affects the outside of the elbow at the lateral epicondyle. The tendinopathy results from overload or repetitive use of the arm, causing an injury similar to
ulnar collateral ligament injury of the elbow
in "pitcher's elbow".
[1]
Description
[
edit
]
The anterior-medial forearm contains several muscles that flex the wrist and
pronate
the forearm.
[1]
These muscles have a common tendinous attachment at the
medial epicondyle of the humerus
at the elbow joint.
[1]
The flexor and pronator muscles of the forearm include the
pronator teres
,
flexor carpi radialis
,
palmaris longus
, and
flexor digitorum superficialis
, all of which originate on the medial epicondyle and are innervated by the
median nerve
.
[1]
The
flexor carpi ulnaris muscle
also inserts on the medial epicondyle and is innervated by the
ulnar nerve
.
[1]
Together, these five muscles have a common attachment (an
enthesis
) on the medial epicondyle of the humerus.
[1]
The flexor tendon is approximately 3 centimetres (1.2 in) long, crosses the medial aspect of the elbow, and runs parallel to the
ulnar collateral ligament
.
[1]
The injury is not acute
inflammation
, but rather is a chronic disorder resulting from overuse of a repetitive arm motion.
[1]
[2]
Repetitive activity leads to recurrent microtears within the flexor tendon, with remodeling of the
collagen
fibers and an increase in the amount of
mucoid
ground substance
.
[1]
As a result, scar tissue formation and thickening of the tendon lead to reduced collagen strength and pain with repetitive use.
[1]
Causes
[
edit
]
 Still shot from a 3D medical animation illustrating golfer's elbow affecting the
medial epicondyle
on the lower inside of the joint.
Still shot from a 3D medical animation illustrating golfer's elbow affecting the
medial epicondyle
on the lower inside of the joint.
The condition is referred to as
golfer's elbow
when a full golf swing causes elbow pain. It may also be called
pitcher's elbow
due to the same tendon being stressed by repetitive throwing of objects, such as a baseball or
football
.
[1]
[3]
[4]
Golfer's elbow appears to occur from repetitive full swings during the period from the top of the backswing to just before ball impact.
[1]
The full swing motion causes high energy
valgus forces
during the late cocking (backswing in golf) and acceleration phase (downswing and impact).
[1]
It is unknown whether this condition is any more common in labor-related occupations with forceful repetitive activities (such as in construction or plumbing) than it is in the general public.
[1]
In adults, the pathophysiology may involve
mucoid
degeneration (disorganized collagen, increased extra-cellular matrix, and chondroid metaplasia).
[5]
Diagnosis
[
edit
]
Medial epicondylitis is diagnosed based on characteristic pain with activities using strength in wrist flexion and confirmed on examination with discrete point tenderness over the common flexor origin at the medial epicondyle, and pain with resisted wrist flexion and passive wrist extension.
[1]
[2]
[4]
[6]
Imaging may be employed, although radiography might show calcifications in the muscle origin.
Ultrasound
and
magnetic resonance imaging
can identify the mucoid degeneration, but are not necessary for diagnosis.
[1]
[2]
[4]
Occurrence
[
edit
]
Medial injury of the flexor tendon is estimated to occur in 0.4% of the population.
[1]
It occurs most often in people ages 45 to 64, is more common in women than in men, and with 75% of cases in the dominant arm.
[1]
Risk factors
for developing golfer's elbow include improper technique or lack of strength, endurance, or flexibility.
[1]
Risk factors in people performing manual labor include heavy and excessive repetition, high
body mass index
, the presence of
comorbidities
, and high work demands.
[1]
Treatment
[
edit
]
Non-specific treatments to alleviate pain include:
[1]
[2]
[4]
Before anesthetics and steroids are used, conservative treatment with an occupational therapist may be attempted. Before therapy can commence, treatment such as rest, ice, compression and elevation (R.I.C.E.) will typically be used.
[1]
[2]
[4]
This will help to decrease the pain and inflammation; rest will alleviate discomfort because golfer's elbow is an overuse injury. The subject can use a tennis elbow splint for compression. A pad can be placed anteromedially on the proximal forearm.
[7]
The splint is made in 30?45 degrees of elbow flexion. A daytime elbow pad also may be useful, by limiting additional trauma to the nerve.
[8]
Simple analgesic medication has a place, as does more specific treatment with oral
anti-inflammatory
medications.
[1]
[2]
[4]
These will help control pain and any inflammation.
[7]
A more invasive treatment is the injection into and around the inflamed and tender area of a
glucocorticoid
(
steroid
) agent.
[9]
Physical therapy
[
edit
]
Therapy includes a variety of exercises for muscle and tendon reconditioning, starting with stretching and gradual strengthening of the flexor-pronator muscles.
[2]
[4]
[6]
Strengthening will slowly begin with
isometrics
and progresses to
eccentric exercises
helping to extend the range of motion back to where it once was. After the strengthening exercises, it is common for the subject to ice the area.
[7]
Surgery
[
edit
]
After 6 months if the symptoms do not improve, surgery may be recommended.
[1]
[2]
[4]
Surgical debridement or cleaning of the area is one of the most common treatments.
[6]
The ulnar nerve may also be decompressed surgically.
[7]
If the appropriate remediation steps are taken ? rest, ice, and rehabilitative exercise and stretching ? recovery may follow. Few subjects will need to progress to steroid injection, and less than 10% will require surgical intervention.
[7]
Arthroscopy
is not an option for treating golfer's elbow.
[6]
See also
[
edit
]
References
[
edit
]
- ^
a
b
c
d
e
f
g
h
i
j
k
l
m
n
o
p
q
r
s
t
u
v
w
x
y
Kiel, John; Kaiser, Kimberly (27 October 2018),
Golfers elbow
, StatPearls Publishing,
PMID
30085542
, retrieved
2019-03-12
- ^
a
b
c
d
e
f
g
h
Childress MA, Beutler A (April 2013).
"Management of chronic tendon injuries"
.
American Family Physician
.
87
(7): 486?90.
PMID
23547590
.
- ^
"Pitcher's Elbow ? Stanford Sports Medicine ? Stanford Medical Outpatient Center"
.
Stanford University Medical Center
. Retrieved
9 September
2009
.
- ^
a
b
c
d
e
f
g
h
Wilson, JJ; Best, TM (1 September 2005).
"Common overuse tendon problems: A review and recommendations for treatment"
.
American Family Physician
.
72
(5): 811?818.
PMID
16156339
.
- ^
Bruni, D.; Pierson, S.; Sarwar, F.; Ring, D.; Ramtin, S. (2023).
"Are the Pathologic Features of Enthesopathy, Tendinopathy, and Labral and Articular Disc Disease Related to Mucoid Degeneration? A Systematic Review"
.
Clinical Orthopaedics and Related Research
.
481
(4): 641?650.
doi
:
10.1097/CORR.0000000000002499
.
PMC
10013668
.
PMID
36563131
.
- ^
a
b
c
d
Amin, Nirav H.; Kumar, Neil S.; Schickendantz, Mark S. (June 2015).
"Medial Epicondylitis: Evaluation and Management"
.
Journal of the American Academy of Orthopaedic Surgeons
.
23
(6): 348?355.
doi
:
10.5435/JAAOS-D-14-00145
.
PMID
26001427
.
S2CID
31827631
.
- ^
a
b
c
d
e
Medial Epicondylitis
at
eMedicine
- ^
"Golfers Elbow | Orthopedic Solutions"
.
orthopedicsolutionsokc.com
.
- ^
Jacobs, J.W.G.; Michels-van Amelsfort, J.M.R. (April 2013). "How to perform local soft-tissue glucocorticoid injections?".
Best Practice & Research Clinical Rheumatology
.
27
(2): 171?194.
doi
:
10.1016/j.berh.2013.03.003
.
PMID
23731930
.
| Classification
| |
|---|
| External resources
| |
|---|
|
|---|
Capsular
joint
| |
|---|
Noncapsular
joint
| |
|---|
| Nonjoint
| |
|---|