Eye condition in which light is focused behind instead of on the retina
"Hyperopia" redirects here. Not to be confused with
Hyperepia
.
Medical condition
| Far-sightedness
|
|---|
| Other names
| Hypermetropia, hyperopia, longsightedness, long-sightedness
[1]
|
|---|
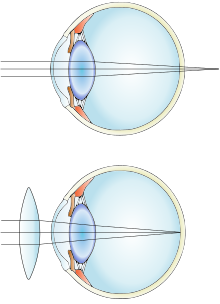 |
| Far-sightedness without (top) and with lens correction (bottom)
|
| Specialty
| Ophthalmology
,
optometry
|
|---|
| Symptoms
| Near blur, Distance and near blur, Asthenopia
[2]
|
|---|
| Complications
| Accommodative dysfunction
,
binocular dysfunction
,
amblyopia
,
strabismus
[3]
|
|---|
| Causes
| Axial length of eyeball is too short, lens or cornea is flatter than normal, aphakia
[2]
|
|---|
| Risk factors
| Ageing, hereditary
[2]
|
|---|
| Diagnostic method
| Eye exam
|
|---|
| Differential diagnosis
| Amblyopia
,
retrobulbar optic neuropathy
,
retinitis pigmentosa sine pigmento
[4]
|
|---|
| Treatment
| Eyeglasses
,
contact lenses
,
refractive surgeries
,
IOL implantation
[2]
|
|---|
| Frequency
| ~7.5% (US)
[5]
|
|---|
Far-sightedness
, also known as
long-sightedness
,
hypermetropia
, and
hyperopia
, is a condition of the
eye
where distant objects are seen clearly but near objects appear blurred. This blur is due to incoming light being focused behind, instead of on, the
retina
due to insufficient
accommodation
by the lens.
[6]
Minor hypermetropia in young patients is usually corrected by their accommodation, without any defects in vision.
[2]
But, due to this accommodative effort for distant vision, people may complain of
eye strain
during prolonged reading.
[2]
[7]
If the hypermetropia is high, there will be defective vision for both distance and near.
[2]
People may also experience
accommodative dysfunction
,
binocular dysfunction
,
amblyopia
, and
strabismus
.
[3]
Newborns are almost invariably hypermetropic, but it gradually decreases as the newborn gets older.
[6]
There are many causes for this condition. It may occur when the axial length of eyeball is too short or if the
lens
or
cornea
is flatter than normal.
[2]
Changes in refractive index of lens, alterations in position of the lens or absence of lens are the other main causes.
[2]
Risk factors include a family history of the condition,
diabetes
, certain medications, and
tumors
around the eye.
[5]
[4]
It is a type of
refractive error
.
[5]
Diagnosis is based on an
eye exam
.
[5]
[8]
Management can occur with
eyeglasses
,
contact lenses
, or refractive corneal surgeries.
[2]
Glasses are easiest while contact lenses can provide a wider
field of vision
.
[2]
Surgery works by changing the shape of the cornea.
[5]
Far-sightedness primarily affects young children, with rates of 8% at 6 years old and 1% at 15 years old.
[9]
It then becomes more common again after the age of 40, known as
presbyopia
, affecting about half of people.
[4]
The best treatment option to correct hypermetropia due to
aphakia
is
IOL
implantation.
[2]
Other common types of refractive errors are
near-sightedness
,
astigmatism
, and
presbyopia
.
[10]
Signs and symptoms
[
edit
]
In young patients, mild hypermetropia may not produce any symptoms.
[2]
The signs and symptoms of far-sightedness include
blurry vision
, frontal or fronto temporal
headaches
,
eye strain
, tiredness of eyes etc.
[2]
The common symptom is eye strain. Difficulty seeing with both eyes (
binocular vision
) may occur, as well as difficulty with depth perception.
[1]
The asthenopic symptoms and near blur are usually seen after close work, especially in the evening or night.
[6]
Complications
[
edit
]
Far-sightedness can have rare complications such as
strabismus
and
amblyopia
. At a young age, severe far-sightedness can cause the child to have double vision as a result of "over-focusing".
[11]
Hypermetropic patients with short axial length are at higher risk of developing
primary angle closure glaucoma
, so, routine
gonioscopy
and glaucoma evaluation is recommended for all hypermetropic adults.
[12]
Causes
[
edit
]
Simple hypermetropia, the most common form of hypermetropia, is caused by normal biological variations in the development of eyeball.
[2]
Aetiologically
, causes of hypermetropia can be classified as:
- Axial: Axial hypermetropia occur when the axial length of eyeball is too short. About 1 mm decrease in axial length cause 3 diopters of hypermetropia.
[2]
One condition that cause axial hypermetropia is nanophthalmos.
[12]
- Curvatural: Curvatural hypermetropia occur when curvature of lens or cornea is flatter than normal. About 1 mm increase in
radius of curvature
results in 6 diopters of hypermetropia.
[2]
Cornea is flatter in microcornea and cornea plana.
[12]
- Index: Age related changes in refractive index (cortical sclerosis) can cause hypermetropia. Another cause of index hypermetropia is diabetes.
[2]
Occasionally, mild hypermetropic shift may be seen in association with cortical or subcapsular cataract also.
[12]
- Positional: Positional hypermetropia occur due to posterior dislocation of Lens or IOL.
[2]
It may occur due to trauma.
[
citation needed
]
- Consecutive: Consecutive hypermetropia occur due to surgical over correction of myopia or surgical under correction in cataract surgery.
[2]
- Functional: Functional hypermetropia results from paralysis of accommodation as seen in internal ophthalmoplegia,
CN III palsy
etc.
[2]
- Absence of lens: Congenital or acquired aphakia cause high degree hypermetropia.
[13]
Far-sightedness is often present from birth, but children have a very flexible eye lens, which helps to compensate.
[14]
In rare instances hyperopia can be due to
diabetes
, and problems with the
blood vessels
in the
retina
.
[1]
Diagnosis
[
edit
]
 Far-sighted vision on left, normal vision on right
Far-sighted vision on left, normal vision on right
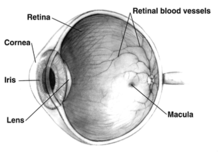 Human eye cross-section
Human eye cross-section
A diagnosis of far-sightedness is made by utilizing either a retinoscope or an automated refractor-objective refraction; or trial lenses in a trial frame or a phoropter to obtain a subjective examination.
Ancillary tests for abnormal structures and physiology can be made via a
slit lamp
test, which examines the cornea,
conjunctiva
, anterior chamber, and
iris
.
[15]
[16]
In severe cases of hyperopia from birth, the brain has difficulty in merging the images that each individual eye sees. This is because the images the brain receives from each eye are always blurred. A child with severe hyperopia can never see objects in detail. If the brain never learns to see objects in detail, then there is a high chance of one eye becoming dominant. The result is that the brain will block the impulses of the non-dominant eye. In contrast, the child with
myopia
can see objects close to the eye in detail and does learn at an early age to see objects in detail.
[
medical citation needed
]
Classification
[
edit
]
 Choroid folds in high hyperopia (fluorescein angiography)
Choroid folds in high hyperopia (fluorescein angiography)
Hyperopia is typically classified according to clinical appearance, its severity, or how it relates to the eye's
accommodative status
.
[
citation needed
]
Clinical classification
[
edit
]
There are three clinical categories of hyperopia.
[3]
- Simple hyperopia
: Occurs naturally due to biological diversity.
- Pathological hyperopia
: Caused by disease, trauma, or abnormal development.
- Functional hyperopia
: Caused by paralysis that interferes eye's ability to accommodate.
Classification according to severity
[
edit
]
There are also three categories severity:
[3]
- Low
:
Refractive error
less than or equal to +2.00
diopters
(D).
- Moderate
: Refractive error greater than +2.00 D up to +5.00 D.
- High
: Refractive error greater than +5.00 D.
Components of hypermetropia
[
edit
]
Accommodation has significant role in hyperopia. Considering accommodative status, hyperopia can be classified as:
[7]
[2]
- Total hypermetropia
: It is the total amount of hyperopia which is obtained after complete relaxation of accommodation using cycloplegics like
atropine
.
- Latent hyperopia
: It is the amount of hyperopia normally corrected by ciliary tone (approximately 1 diopter).
- Manifest hyperopia
: It is the amount of hyperopia not corrected by ciliary tone. Manifest hyperopia is further classified into two, facultative and absolute.
- Facultative hyperopia
: It is the part of hyperopia corrected by patient's accommodation.
- Absolute hyperopia
: It is the residual part of hyperopia which causes blurring of vision for distance.
So, Total hyperopia= latent hyperopia + manifest hyperopia (facultative + absolute)
[7]
Treatment
[
edit
]
Corrective lenses
[
edit
]
The simplest form of treatment for far-sightedness is the use of
corrective lenses
, i.e. eyeglasses or contact lenses.
[17]
[18]
Eyeglasses used to correct far-sightedness have
convex lenses
.
[19]
Surgery
[
edit
]
There are also surgical treatments for far-sightedness:
Laser procedures
- Photorefractive keratectomy
(PRK): This is a refractive technique that is done by removal of a minimal amount of the corneal surface.
[19]
[20]
Hyperopic PRK has many complications like regression effect, astigmatism due to epithelial healing, and corneal haze.
[21]
Post operative epithelial healing time is also more for PRK.
[22]
- Laser assisted in situ keratomileusis
(LASIK): Laser eye surgery to reshape the cornea, so that glasses or contact lenses are no longer needed.
[20]
[23]
Excimer laser LASIK can correct hypermetropia up to +6 diopters.
[21]
LASIK is contraindicated in patients with
lupus
and
rheumatoid arthritis
.
[21]
- Laser epithelial keratomileusis (LASEK): Resembles PRK, but uses alcohol to loosen the corneal surface.
[19]
- Epi-LASIK:
Epi-LASIK
is also used to correct hyperopia.
[22]
In this procedure, use of epikeratome eliminates the use of alcohol.
[22]
- Laser thermal keratoplasty (LTK):
Laser thermal keratoplasty
is a laser based non-destructive refractive procedure used to correct hyperopia and presbyopia.
[22]
It uses Thallium-Holmium-Chromium (THC): YAG laser.
[22]
IOL implantation
- Aphakia correction: High degree hypermetropia due to absence of lens (aphakia) is best corrected using intraocular lens implantation.
[
citation needed
]
- Refractive lens exchange (RLE): A variation of
cataract surgery
where the natural
crystalline lens
is replaced with an artificial
intraocular lens
; the difference is the existence of abnormal ocular anatomy which causes a high refractive error.
[24]
- Phakic IOL:
Phakic intraocular lens
are lenses that implanted inside eye without removing the normal crystalline lens. Phakic IOLs can be used to correct hypermetropia up to +20 diopters.
[22]
Non laser procedures
- Conductive keratoplasty (CK):
Conductive keratoplasty
is a non laser refractive procedure used to correct presbyopia and low hypermetropia (+0.75D to +3.25D) with or without astigmatism (up to 0.75D).
[22]
[25]
It uses radiofrequency energy to heat and shrink corneal collagen tissue. CK is contraindicated in pregnant/breastfeeding women, central
corneal dystrophies
and
scarring
, history of
herpetic keratitis
, type 1 diabetes etc.
[25]
- Automated lamellar keratoplasty (ALK): Hyperopic
automated lamellar keratoplasty
(H-ALK) and Homoplastic ALK are ALK procedures that corrects low to moderate hyperopia.
[26]
Poor predictability and the risk of complications limits usefulness of these procedures.
[26]
- Keratophakia and epi-keratophakia are another two non laser surgical procedures used to correct hypermetropia.
[26]
Keratophakia is a surgical technique developed by Barraquer for treating high hypermetropia and aphakia. Poor predictability and induced irregular
astigmatism
are complications of these procedures.
[26]
Etymology
[
edit
]
The term
hyperopia
comes from
Greek
?π?ρ
hyper
"under and ?ψ
?ps
"sight" (
GEN
?π??
?pos
).
[27]
References
[
edit
]
- ^
a
b
c
Lowth, Mary.
"Long Sight (Hypermetropia)"
.
Patient
. Patient Platform Limited.
Archived
from the original on 2016-03-03
. Retrieved
2016-02-26
.
- ^
a
b
c
d
e
f
g
h
i
j
k
l
m
n
o
p
q
r
s
t
u
v
Khurana, AK (September 2008). "Errors of refraction and binocular optical defects".
Theory and practice of optics and refraction
(2nd ed.). Elsevier. pp. 62?66.
ISBN
978-81-312-1132-8
.
- ^
a
b
c
d
Moore, Bruce D.; Augsburger, Arol R.; Ciner, Elise B.; Cockrell, David A.; Fern, Karen D.; Harb, Elise (2008).
"Optometric Clinical Practice Guideline: Care of the Patient with Hyperopia"
(PDF)
.
American Optometric Association
. pp. 2?3, 10?11. Archived from
the original
(PDF)
on 2006-07-17
. Retrieved
2006-06-18
.
- ^
a
b
c
Kaiser, Peter K.; Friedman, Neil J.; II, Roberto Pineda (2014).
The Massachusetts Eye and Ear Infirmary Illustrated Manual of Ophthalmology E-Book
. Elsevier Health Sciences. p. 541.
ISBN
9780323225274
.
Archived
from the original on 2017-09-08.
- ^
a
b
c
d
e
"Facts About Hyperopia"
.
NEI
. July 2016. Archived from
the original
on 8 July 2017
. Retrieved
11 July
2017
.
- ^
a
b
c
Ramjit, Sihota; Radhika, Tandon (15 July 2015). "Refractive errors of the eye".
Parsons' diseases of the eye
(22nd ed.). Elsevier.
ISBN
978-81-312-3818-9
.
- ^
a
b
c
Pablo, Artal (2017).
Handbook of visual optics-Fundamentals and eye optics and
. CRC Press.
ISBN
978-1-4822-3785-6
.
- ^
Eye Examination Guide
- ^
Castagno, VD; Fassa, AG; Carret, ML; Vilela, MA; Meucci, RD (23 December 2014).
"Hyperopia: a meta-analysis of prevalence and a review of associated factors among school-aged children"
.
BMC Ophthalmology
.
14
: 163.
doi
:
10.1186/1471-2415-14-163
.
PMC
4391667
.
PMID
25539893
.
- ^
"Facts About Refractive Errors"
.
National Eye Institute
. October 2010.
Archived
from the original on 28 July 2016
. Retrieved
30 July
2016
.
- ^
"Complications of long-sightedness"
.
NHS Choices
. National Health Service. 2014-07-09. Archived from
the original
on 2016-03-05
. Retrieved
2016-02-26
.
- ^
a
b
c
d
John F., Salmon (2020).
Kanski's clinical ophthalmology: a systematic approach
(9th ed.). Edinburgh: Elsevier.
ISBN
978-0-7020-7713-5
.
OCLC
1131846767
.
- ^
Khurana, AK (2015). "Errors of refraction and accommodation".
Comprehensive ophthalmology
(6th ed.). Jaypee, The Health Sciences Publisher. pp. 37?38.
ISBN
978-93-86056-59-7
.
- ^
"Normal, near-sightedness, and far-sightedness"
.
MedlinePlus Medical Encyclopedia
.
Archived
from the original on 2016-03-05
. Retrieved
2016-02-26
.
- ^
"Farsightedness"
.
MedlinePlus Medical Encyclopedia
.
Archived
from the original on 2016-02-24
. Retrieved
2016-02-26
.
- ^
"Slit-lamp exam"
.
MedlinePlus Medical Encyclopedia
.
Archived
from the original on 2016-03-05
. Retrieved
2016-02-26
.
- ^
Chou, Roger; Dana, Tracy; Bougatsos, Christina (2011-02-01).
"Introduction"
.
Screening for Visual Impairment in Children Ages 1-5 Years: Systematic Review to Update the 2004 U.S. Preventive Services Task Force Recommendation
(Report). Evidence Syntheses. Vol. 81. Rockville, MD: Agency for Healthcare Research and Quality.
PMID
21542544
.
Archived
from the original on 2017-09-08 – via PubMed Health.
- ^
"Farsightedness (Hyperopia): Treatments"
.
PubMed Health
. U. S. National Library of Medicine.
Archived
from the original on 2017-09-08
. Retrieved
2016-02-26
.
- ^
a
b
c
"Treating long-sightedness"
.
NHS Choices
. National Health Service. Archived from
the original
on 2016-03-05
. Retrieved
2016-02-26
.
- ^
a
b
Settas, George; Settas, Clare; Minos, Evangelos; Yeung, Ian Yl (2012-01-01).
"Photorefractive keratectomy (PRK) versus laser assisted in situ keratomileusis (LASIK) for hyperopia correction"
.
Cochrane Database of Systematic Reviews
.
6
(6): CD007112.
doi
:
10.1002/14651858.CD007112.pub3
.
ISSN
1469-493X
.
PMC
7388917
.
PMID
22696365
.
- ^
a
b
c
Gulani, Arun C (9 November 2019).
"LASIK Hyperopia: Background, History of the Procedure, Problem"
.
- ^
a
b
c
d
e
f
g
Khurana, AK (September 2008). "Refractive surgery".
Theory and practice of optics and refraction
(2nd ed.). Elsevier. pp. 307?348.
ISBN
978-81-312-1132-8
.
- ^
"Laser Eye Surgery"
.
MedlinePlus
.
Archived
from the original on 2016-03-06
. Retrieved
2016-02-26
.
- ^
Alio, Jorge L.; Grzybowski, Andrzej; Romaniuk, Dorota (2014-12-10).
"Refractive lens exchange in modern practice: when and when not to do it?"
.
Eye and Vision
.
1
: 10.
doi
:
10.1186/s40662-014-0010-2
.
ISSN
2326-0254
.
PMC
4655463
.
PMID
26605356
.

- ^
a
b
"Conductive Keratoplasty"
.
eyewiki.aao.org
.
- ^
a
b
c
d
Refractive surgery
. Azar, Dimitri T. (2nd ed.). Philadelphia: Mosby / Elsevier. 2007.
ISBN
978-0-323-03599-6
.
OCLC
853286620
.
{{
cite book
}}
: CS1 maint: others (
link
)
- ^
"hyperopia"
.
Online Etymology Dictionary
. Douglas Harper.
Archived
from the original on 2017-09-08.
External links
[
edit
]
| Classification
| |
|---|
| External resources
| |
|---|